
In a terrifying show of crowd psychology, berserk governments are destroying their countries to extend the lives of a very few people for a few months. The cause of this madness is the WHO/ UK’s Imperial College March 19 Report. That its assumptions have been shown to be wrong is having no effect on headlong suicidal policies being pursued.
Read its fine print. “Suppression…carries with it enormous social and economic costs which may themselves have significant impact on health and well-being in the short and longer-term.” “We do not consider the ethical or economic implications of either strategy [mitigation or suppression] here…” * And by the way, WHAT IS the mortality rate??
Their assumption was that 80% would become infected, the infection fatality rate would be 0.9%, so 0.7% of the population would die over 2 years, the majority in 2020. Enough months of shutdown to be economic suicide would theoretically “save” half of these. This was the source of every official fear mongering statement and every scary headline. Even as evidence piled up that none of this was correct, governments sowed panic and launched scorched earth policies that will now cause more deaths over time than Covid.
Covid is not the Spanish flu, which afflicted the young and healthy. The UK report gives age cohort IFRs, from a 0.03% probability of dying for ages 20 to 29, to 9.3% for ages over 80. Using their cohort IFRs and population age data, one can calculate that roughly 90%of deaths would be of those over 60, and 70% to 80% would be those over 70.
Why did they not point this out?
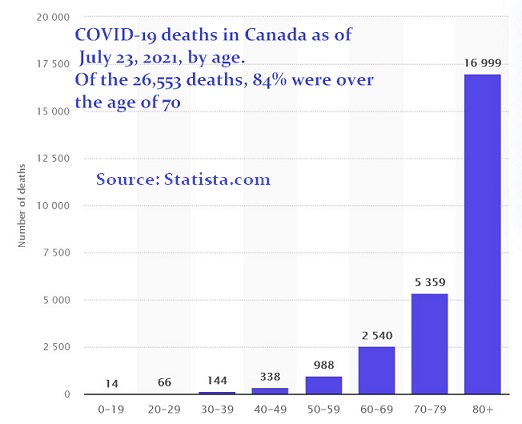
As of fall 2020, the average age of Canadian Covid deceased was 84 years. An 80 year old already has over a 20% chance of dying in the next 2 years, a 90 year old, nearly 40%. Thus the projected deaths include many who would have died of something else. Not to mention the ethical problem of anti-Covid measures that attempt to extend the lives of the elderly by throwing their children under the bus. By June 2021, all of 26,553 Canadian covid deaths were recorded. Approximately 1,000 Canadians die every day as part of normal mortality. In this approximately 18 month period some 540,00 deaths occurred.
To imply that the above deaths were all incremental was just wrong. (To relax, read A Mathematician Reads the Newspaper by J.A.Paulos.)
Infection Fatality Rate
The Center for Disease control planned on 0.46% for symptomatic people (which includes a rate of only 0.2% to 0.05% risk for those under 65 and a 1.3% rate for those over 65.
Note: A 70 year old already has an over 2% risk of dying!)
Even their worst case scenario has the risk for those under 65 at only 0.1% to 0.6%). And counting asymptomatic people lowers 0.46% to 0.26%. This paper was updated 10 September but the age cohorts were changed, the weighted average not given, but the averages could be similar.
Other Opinions on the IFR
At Stanford, Prof. John Ioannidis arrived numbers similar to the CDC’s first version, around a quarter of one percent. “Deaths for people <65 years without underlying predisposing conditions are remarkably uncommon.” “For someone under 65 with no underlying conditions, the risk is completely negligible.”
He also pointed out that different coronaviruses infect millions of people every year, and they are common especially in the elderly and in hospitalized patients with respiratory illness in the winter. Case fatality of 8% has been described in outbreaks among nursing home elderly in the past, AND the average mortality rate in nursing homes is 30% even without Covid.
Recent data show that the vast majority of carriers have no or only mild symptoms, and show that the number of infected people is far greater than expected, i.e., the fatality rate is far lower than originally assumed.
Professor Johan Giesecke, M.Sc., M.D., Ph.D., a former State Epidemiologist in Sweden said, “I think it would be like a severe influenza season, the same as, and which would be an order of 0.1 percent maybe.”
Professor Hendrik Streek estimated the IFR in a heavily affected German town to be only 0.36%.
The risk for young people is comparable to the flu. Dr. David L. Katz mentioned that the flu is more lethal to children than Covid-19. (See sites, and more at the end of this post.)
On the other hand, if PCR+ves are the denominator, the IFR may be understated. One article claimed Covid was 3 times more lethal than the flu (not that averages, given steep risk gradient by age, have much use).
Suppose Covid-19 is 3x worse than the flu. This is not ebola! It is still widely accepted that the vast majority easily survive Covid. Would any sane person collapse the economy, destroy small businesses, issue stay-home orders, put masks on healthy people, because a disease that was only 3x worse than the flu was circulating?
Testing, Testing, Testing
There are hitches in calculating the rate. Reliable testing is required. This took time. (Before there were any tests, and Covid overlapped with late flu season, it is thought that many deaths may have been incorrectly ascribed to Covid.)
Beda Stadler, Prof Emeritus, Immunology, Med Faculty Univ of Switzerland said,
” The [+ve PCR] test does not tell you if you have the virus or some dead chunk of the virus. It does not tell you if it is virulent. No other virus has been accompanied by so much testing and testing has created so much nonsense and panic.”
Number of Cases Rising!!! Panic! Panic!
Dramatic headlines listing numbers of Covid deaths without context are irresponsible . Most of these are found simply because more are tested. Since the vast majority will recover, many will have no symptoms, and some, according to many, do have some immunity, this is not a bad thing. As a doctor said, “Eventually we’ll all get it.”
The PCR CaseEdemic
The PCR test was invented some years ago and it was considered a boon for paleo-biology, genetics, biology…but not for diagnosing disease. None of the wholesale destruction of businesses, people’s lives & government finances would have taken place without the PCR test. It may be a good thing that its Nobel Laureate inventor did not live to see Covid-19. Dr. Simone Gold at the July 2020 America’s Frontline Doctors interview said:
“If you told us a few months ago that the media would go hysterical at the number of “cases” we’d have laughed. Most have few or no symptoms.”
The Drosten PCR test is SO FLAWED that 20 scientists wrote the Eurosurveillance Board to have a paper supporting it withdrawn. A key complaint was that it was, by itself, not a diagnostic tool for disease.
Unless an article specifies that these are reported cases requiring hospitalization, it is meaningless. Yet governments are incompetently and destructively basing policy on these tests. Their rational is the belief that +ve tests presage deaths and hospitalizations. They do not. In the US and in Europe it is notable that while +ve tests rise, deaths and hospitalizations are declining.
In Ontario, the cycle threshold used is so high, that essentially none of the “cases” are infected or infectious. See more about the JCCF‘s fine work on this.
The Media Uses 1984 NewsSpeak
In the past, the CDC required there be symptoms, before someone was called a “case”. The CDC tried to re-establish this in the second half of 2020 by advising that asymptomatic people NOT be tested. They were forced to backtrack by the media, politicians and medical bureaucrats. Now, not only does the media call positive PCR tests “cases”, it even refers to them as “infections”. Yes, our tax-supported CBC is essentially lying to us.
80% will get it….or is it more like 20%
So much for the original assumption that 80% will be infected.
Dr. Karol Sikora said there are other immune responses besides antibodies, the mucosal membrane for one, “that do not leave a footprint for a test….we should not assume that no antibodies means no exposure”.
Dr. Dolores Cahill, who researched antibodies, also mentions this alternative response.
Dr. Katz added that in sequestered groups such as cruise ships, naval vessels, there seemed to be constant percentage, only 20% who would get infected. He added that this could mean we are much closer to herd immunity than previously thought.
Professor Karl Friston, a prominent member of the independent SAGE committee, set up by Sir David King to challenge government scientific advice — comes a claim that the true portion of people who are not even susceptible to COVID-19 may be as high as 80%.
A recent BMJ article says that that the majority of people under 20, when exposed to the virus, do not get infected. They and many others flick off the virus using non-specific T cells and other immunity tools.
Immunologist Beda Stadler said: “70 – 80 percent of the people are most likely immune.”
Not long ago, this was considered Covid denialism. Now some prior resistance and immunity to COVID-19 is becoming accepted scientific fact. (Sites below.)
What does this do to the fatality rate?
The Infection Fatality Rate was first assumed to be more or less the same as the fatality rate among all those exposed. Now we know it is not because many exposed people took in the virus but were not infected. So the risk is really best measured by Exposure Fatality Rate.
And this could well be a tiny fraction of earlier numbers, 0.26% to 0.65%.
R0 and Exponential Spread?
The Imperial College disregarded these first line defenses (which are studied in Human Biology 101) and they assumed no one had innate immunity. So, they assumed the R0, the number of additional infections from one person was around 2.4 and that it stayed constant and that cases multiplied exponentially.
According to experts it does not spread that way. As explained by Dr. Michael Levitt of Stanford, the spread was never going to be exponential, and that the growth rate begins to slow after two weeks.
This was backed up by Dr. Knut Wittkowski, retired epidemiologist, and Prof Isaac Ben-Israel.
Dr. Sikora says the decline in infection rates are NOT just from social distancing and attributed the decline to the other immune responses.
Others have surmised that changes in viruses could also be behind the typical pattern of spread.
Comments on the Imperial College Report
In an interview with Stanford’s (very diplomatic) Dr. Ioannidis, an interviewer asked him about this:
The Imperial College/ Neil Ferguson originally projected 500,000 UK deaths. The Oxford study took issue with it. Neil Ferguson changed it down to 20,000 [a 96% reduction!], and said it was due to social distancing -which had only been in place for one day. [The sceptical expression on Dr. Ioannidis’ face in response to this says it all.]
How could the very smart Imperial College/ WHO have made mistakes of this magnitude?
Ioannidis: They worked under stressful conditions with limited evidence. so they assumed the worst the default option. They got it astronomically wrong, that is indeed the case. Those predictions of millions of [US] deaths were science fiction. Our California research and others shows the IFR to be very low.
Dr. Knut Wittkowski also rejected the idea that social distancing had caused this difference.
Professor Beda Stadler said,
“Whatever a country did did not matter. The curves were coming down, so that means that all the model calculators, epidemiologist with their self-made computer programs, that was basically bullshit, because there was a basic immunity there.”
[So why is anyone still listening to the WHO?]
A Tragedy of Errors?
Professor Gieseke also pointed out that “the Imperial College paper was never published – scientifically – it’s not peer-reviewed, which scientific paper should be.” Peter St. Onge of the Montreal Economic Institute wrote an excellent article that chronicles the history of errors in the Imperial College Report.
The WHO is now furiously backtracking., Rather than admit the original projections are nowhere near reality, it is crediting the shutdown to save face. All shutdown measures could been dropped immediately. Instead, the WHO and allied governments prefer to prolong anti-Covid measures rather than to admit mistakes. We now know about the number of asymptomatic carriers, and how the virus survives on surfaces, and we know what unbiased experts can tell us: mitigation and quarantine could not possibly account for the reduction in numbers.
WHODUNIT?
Why people do NOT trust the WHO.
They lost their opportunity to correct their work early by blaming lack of data. The more they clung to their projections, which were nowhere near reality, the worse it was. THAT is why the WHO continues to spread fear and urge extreme measures, masks, distancing.
If they can convince naïve Chief Medical Officers (who are getting dictatorial powers these days) to implement strict measure, the WHO can credit those measures for subsidence in infection rates, however implausible, and never admit their mistakes, even though this trend is natural and has been seen before. And if feckless politicians believe them, they will happily destroy the country.
An Example of the WHO’s bias was in a July National Post article (site below):
‘The WHO “has amended it’s assessment and said Swedish contagion rates are in fact stable. It linked the high number of cases to an increase in testing.” This is after Sweden had to lambaste the organization for making a “total mistake”!
How many mistakes have to come out of WHO before we realize EVERY directive coming from them has a political motive?‘
Newsflash! The WHO Casually Makes an Impromptu Major Correction!
Maria van Kerkhove, PhD and WHO epidemiologist said in a June 8th press conference that it was very rare that they found transmission of the virus from asymptomatic cases. Transmission from people not sick was the the entire raison d’être for face masks and distancing.
So what did they do? They waffled, they prevaricated, they flummeried, etc. Moreover, the transmission by asymptomatic and pre-symptomatic people could hardly be considered unusual in infectious diseases. As usual, good news Must Be Suppressed in the interest of destroying jobs and businesses. If you’re wondering when the WORLD HEALTH ORG. will decide to tell the governments they just need to let the virus do its thing… that is probably never. Saving face is more important.
What about flattening the curve? As of early August 2020, at least one Toronto hospital had NO Covid patients. Instead of dealing with infections in the quieter summer months, any outbreak will now be pushed into the next flu season. It is known that these things come in waves. Governments did nothing to add to staff and facilities in 2020, so in 2021, they locked down again to protect the already inadequate health care facilities
What about plangent tales of statistically insignificant cases of young people with Covid? Decisions need to be rational, not emotional. Covid is a relatively benign disease for the young. Ever wonder why mainstream media never mentions how few young people become ill? Do we throw one million out of work to postpone fatal infection of one 25 year old with pre-existing conditions? Did your newspaper write about the 100 year old who easily recovered from Covid.
The better the news on fatality rates and contagion, the more intransigent are governments. Instead of rejoicing they still instill fear, with the media’s help, to get compliance. Young people, whose risk is trivial, are cowering in masks. People shun their neighbours. All this is for a virus with less than a 1 in a 1,000 probability of killing a 35 year old. If this scorched earth policy continues, the apocalyptic Great Depression of 2020 will go down as one of the greatest follies of all time.

“Zero effort was dedicated to establishing whether the trillions of dollars in economic loss [and] unprecedented disruption in the lives of billions of people were justifiable.” -Terence Corcoran, National Post, 25 June 2020
No matter what is done, Covid will be the cause of many deaths. It is the refusal to accept this that drives the frantic behaviour. We need leaders who WILL consider the economic and human costs that the UK Report omits, and who WILL tell the truth. People are going to die. Get over it. Staying home is not a solution, and nor is putting every healthy person in a mask.
As professor Ioannidis said, “I think that there is a risk of really making some fundamental decisions about the structure of our civilization, of our society, of our future, that may not be appropriate.” As an example, he cited the risks of constructing a society over the longer term around where everything is done at a distance. And as Prof. Michael Levitt put it: “There is no doubt in my mind, that when we come to look back on this, the damage done by lockdown will exceed any saving of lives by a huge factor.
Most boomers would gladly give up a few years of life to ensure their children’s future, and we need to be heard. Destructive shutdown or face masks, distancing and a culture of fear are not just a medical decision. It is for economists, actuaries, ethicists and people who care about the young and the working class to decide, for the greatest good for the greatest number.
SITES for reference & further reading
PCR Tests in Manitoba -Justice Centre for Constitutional Freedoms 11 May 2021
(The JCCF is a tax-receipt issuing Canadian charity.)
https://www.jccf.ca/manitoba-chief-microbiologist-and-laboratory-specialist-56-of-positive-cases-are-not-infectious/
Michael Yeadon, PhD, formerly VP and scientist at Pfizer, on PCR tests and more
Retraction request re: the Drosten PCR test
https://2020news.de/en/drosten-pcr-test-study-withdrawal-requested-due-to-scientific-error-and-massive-conflict-of-interest/
More opinions at:
https://www.canadianhealthpolicy.com/blog/covid-19-dissenting-opinions.html
Including an article by 2 Canadian infectious disease experts, Drs Neil Rau & Susan Richardson “This sledgehammer approach will affect mainly able- bodied workers, children and students, for whom a COVID-19 infection will be nothing more than a cold. It will put a huge segment of the workplace out of commission, including healthcare workers, at a time when we need them most.”
Dr. Knut Wittkowski [highly recommended] : There are many people supporting my positions; they are not favored by the media, [for] the media—only bad news is good news…[T]he huge damage done to the economy could not be justified by whatever was known.
https://21stcenturywire.com/2020/05/01/coronavirus-epidemiologist-dr-knut-wittkowski-lockdown-has-no-benefit-only-negative-effects/
An professional blog with links to academic sources, HOWEVER,
Facebook warns this site is “inaccurate”. FB’s 2 main complaints are its IFR that is much lower than “official” sources, and the site’s description of existing non-specific immunity. This latter complaint seems baseless, given how many respectable professionals support it. The IFR may be overly optimistic, but the WHO is not censored for errors, so, let us not censor this.
https://swprs.org/a-swiss-doctor-on-covid-19/
Another good blog is at Dryburgh.com –
Antibodies
https://www.medscape.com/viewarticle/932671
COVID-19 Antibodies Can Disappear After 2-3 Months, Study Shows
Scientists in China studied 74 people with coronavirus, half symptomatic, half asymptomatic. Eight weeks after recovery, antibody levels fell to undetectable levels in 40% of asymptomatic people
British Professor Karol Sikora, MD, & former head of the WHO’s cancer program
https://www.medscape.com/viewarticle/930977
https://unherd.com/thepost/professor-karol-sikora-fear-is-more-dangerous-than-the-virus/
Professor Michael Levitt, Stanford School of Medicine,
https://unherd.com/thepost/nobel-prize-winning-scientist-the-covid-19-epidemic-was-never-exponential/
2 May 2020 “[E]xponential growth in infection… hasn’t actually happened anywhere, even in countries relatively lax in their responses.” “I think the policy of herd immunity is the right policy.
I think Britain was on exactly the right track before they were fed wrong numbers.
And they made a huge mistake [in going with lockdown].”
Professor Karl Friston on rate of spread and immunity
https://unherd.com/2020/06/karl-friston-up-to-80-not-even-susceptible-to-covid-19/
Beda Stadler, Prof Emeritus, Immunology, Med Faculty Univ of Switz.
On Immunity, Spread, Testing, and ‘Is the virus ‘novel?”‘
Interview with Ivor Cummins, 28 July 2020
https://www.youtube.com/watch?v=GBRcK-od50Q
“…all over Europe the curve came down & independent of whether there was harsh lockdown or not. Whatever a country did did not matter.”
Oxford Epidemiologist Sunetra Gupta
https://www.dailywire.com/news/oxford-epidemiologist-heres-why-that-doomsday-model-is-likely-way-off
“I am surprised that there has been such unqualified acceptance of the Imperial model,” Dr. Sunetra’s researchers believe both the hospitalization and mortality rates are much lower than the worst estimates, and immunity is more widespread than previously thought.
https://www.express.co.uk/news/science/1257162/Coronavirus-symptoms-COVID19-infected-no-symptoms-latest-coronavirus-news
According to Professor Adam Antczak from the Medical University of Łódź, Poland, the coronavirus only infects a small slice of the infected populace with severe symptoms.”This means that as much as 80 percent of infected people do not show symptoms of the disease or suffer from mild or moderate illness, that is, similar to the common cold.”
Dr. David Katz on Medscape https://www.medscape.org/viewarticle/930482 and other sites
Professor Hendrik Streeck of the Institute of Virology, University of Bonn, Germany
With the seven SARS-CoV-2-associated reported deaths the estimated IFR was 0.36%. The unexpectedly low secondary infection risk among persons living in the same household has important implications for measures installed to contain the SARS-CoV-2 virus pandemic.
Abstract https://www.medrxiv.org/content/10.1101/2020.05.04.20090076v2
also at https://doi.org/10.1101/2020.05.04.20090076
CDC REDUCES IFR to something like a really bad seasonal flu
Discussion
https://thevaccinereaction.org/2020/06/cdc-reduces-covid-19-fatality-rate-to-0-26-percent/
CDC report itself, updated
https://www.cdc.gov/coronavirus/2019-ncov/hcp/planning-scenarios.html#five-scenarios
Professor Johan Giesecke, M.Sc., M.D., Ph.D., the State Epidemiologist from 1995 to 2005 and a leading consultant on the Swedish model. Interviewed by Edward Peter Stringham
https://www.aier.org/article/lockdown-free-sweden-had-it-right-says-world-health-organization-interview-with-prof-johan-giesecke/ 30 April 2020
Dr. John Ioannidis, Stanford
https://nationalpost.com/opinion/munk-debates-were-making-high-stakes-covid-19-decisions-without-reliable- data
27 March 2020. “The Iceland experience and other data from Rome and Italy where entire city populations were tested shows that the vast majority of people are either completely asymptomatic or mildly symptomatic in ways that you would not be able to differentiate from the common cold or common flu. This information makes a huge difference while we are proceeding with aggressive measures of social distancing and lockdowns that may have tremendous repercussions, especially in the long term.”
also
https://thevaccinereaction.org/2020/04/perspectives-on-the-pandemic-dr-john-ioannidis/ Interview
Dr. John Ioannidis 4-8 April 2020 Papers on mortality risk
https://www.medrxiv.org/content/10.1101/2020.04.05.20054361v1
https://doi.org/10.1101/2020.04.05.20054361
https://www.medrxiv.org/content/10.1101/2020.05.13.20101253v3
“The COVID-19 death risk in people <65 years old during the period of fatalities from the epidemic was equivalent to the death risk from driving between 9 miles per day and 415 miles per day.”
BMJ on Infection Susceptibility Infection Rates in Youth
Covid-19: Researchers question policy of closing schools after finding under 20s have low susceptibility to virus
https://www.bmj.com/content/369/bmj.m2439 17 June 2020 Cite as: BMJ 2020;369:m2439
https://doi.org/10.1136/bmj.m2439
Original article by N.G.Davies, Dept. of Infectious Disease Epidemiology,
London Sch. of Hygiene & Tropical Medicine, UK
https://www.nature.com/articles/s41591-020-0962-9 original article
Dr. Dolores Cahill
https://gumshoenews.com/2020/05/14/professor-dolores-cahill-debunking-of-the-corona-narrative/
https://www.bitchute.com/video/Avc6_ftzk3w/
Professor Daniel B. Kline, economist
https://www.aier.org/article/municipality-second-waves-zero-and-counting/
“In talking of a second wave, the unit of analysis should be COVID deaths (or, if we must, hospitalizations), not test-positive cases. When more tests are done, more cases are found.”
Article has graphs of declining deaths & hospitalizations in the US.
Peter St. Onge a senior fellow at the Montreal Economic Institute.
The worst-case scenario that closed Canada National Post (Latest Edition) 25 Jun 2020
https://www.iedm.org/fr/the-worst-case-scenario-that-closed-canada/
“Covid has killed far fewer Canadians under 35 than traffic accidents normally do.” “Professor Neil Ferguson [leader of the Imperial College team] has a history of hysterically over-predicting deaths from new diseases.”
The WHO Backtracks on Sweden by Suzanne Reny, 2 July 2020
https://nationalpost.com/news/canada/swedish-covid-expert-says-the-world-still-doesnt-understand
America’s Frontline Doctors Interview. (More on this in the Censorship post.)
https://www.bitchute.com/video/Gnw3ptigEj8B/
https://www.rev.com/blog/transcripts/americas-frontline-doctors-scotus-press-conference-transcript
Drs Dan Erickson and Artin Massihi,
It is often repeated that these doctors’ methodology was seriously flawed.
The reference is left here in fairness, since the WHO’S report was found to have major flaws but they are not censored.
also at https://www.dailymotion.com/video/x7tkx22 Dan Erickson and Artin Massihi,
https://www.thegatewaypundit.com/2020/05/dr-erickson-warns-soros-wants-government-take-youtube-facebook-video-removed-youtube
